The tricep muscle is rarely the first structure clinicians reference when discussing upper body strength and longevity — yet its mass, function, and rate of atrophy are directly implicated in sarcopenia progression, insulin-mediated glucose disposal, and long-term functional independence. For executives and founders tracking healthspan variables, the tricep represents more than an aesthetic marker. As the largest muscle group in the upper arm, comprising approximately two-thirds of total upper arm mass, tricep integrity correlates with grip strength trajectories, resting metabolic rate, and the kind of neuromuscular reserve that determines physical capacity well into the sixth and seventh decades.
Tricep Anatomy: A Functional Overview
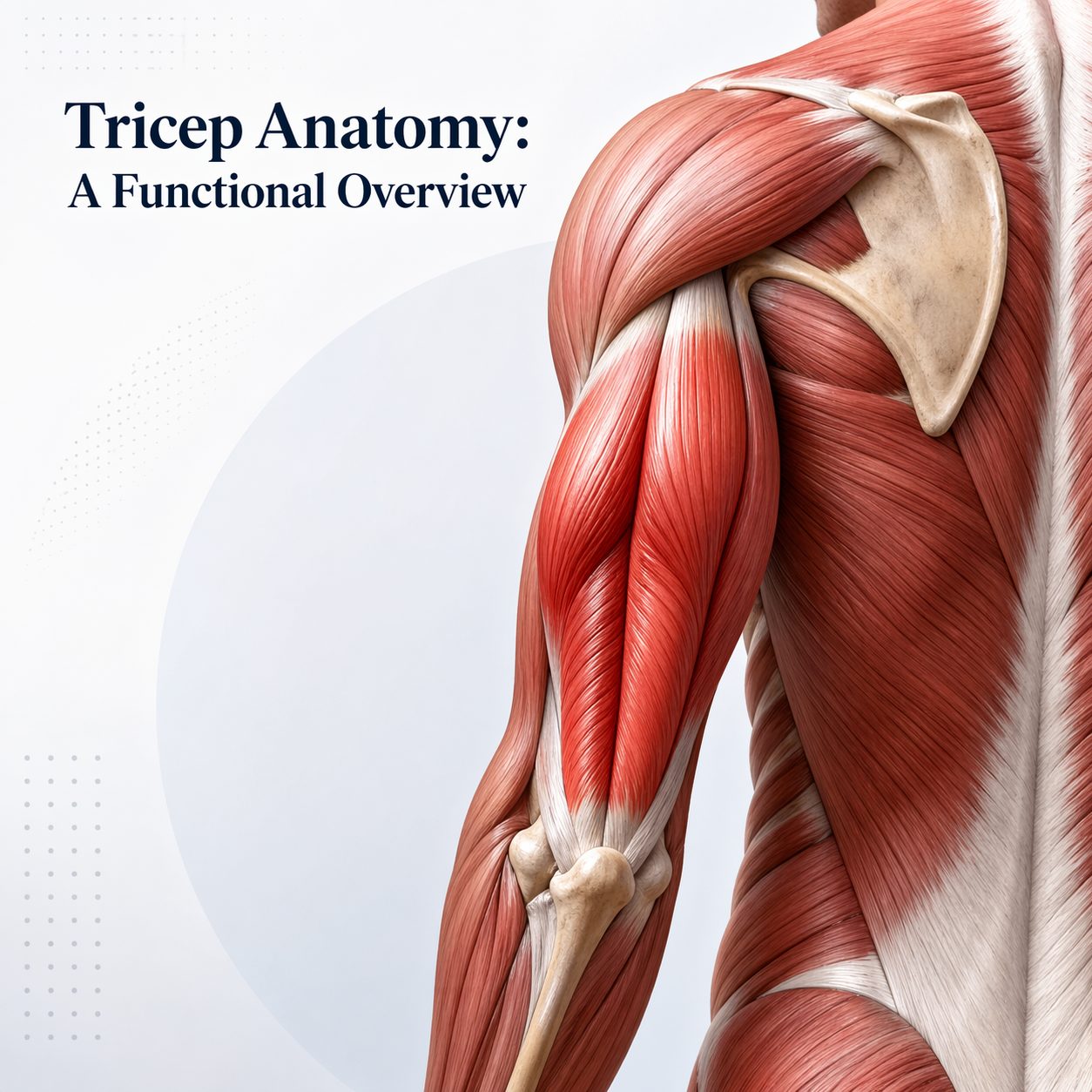
The tricep muscle — formally the triceps brachii — is a three-headed muscle on the back of the upper arm. Its three heads are the long head, originating from the shoulder blade, and the lateral and medial heads, both originating from the back of the upper arm bone. All three converge into a single tendon attaching at the olecranon — the bony point of the elbow. This structure gives the tricep its primary function: straightening the elbow.
Beyond elbow extension, the long head crosses the shoulder joint. This makes it a contributor to shoulder movement and stability — not merely a pushing muscle. Its role in shoulder joint integrity is often underappreciated in both clinical and performance settings.
Understanding this anatomy clarifies why tricep decline carries consequences beyond reduced pushing strength. Shoulder instability, poor posture, and increased strain on the rotator cuff all follow from long head weakness. For professionals spending significant time at desks or traveling, these structural vulnerabilities build silently over years before surfacing as pain or limited movement.
Tricep Muscle Mass and Sarcopenia Progression
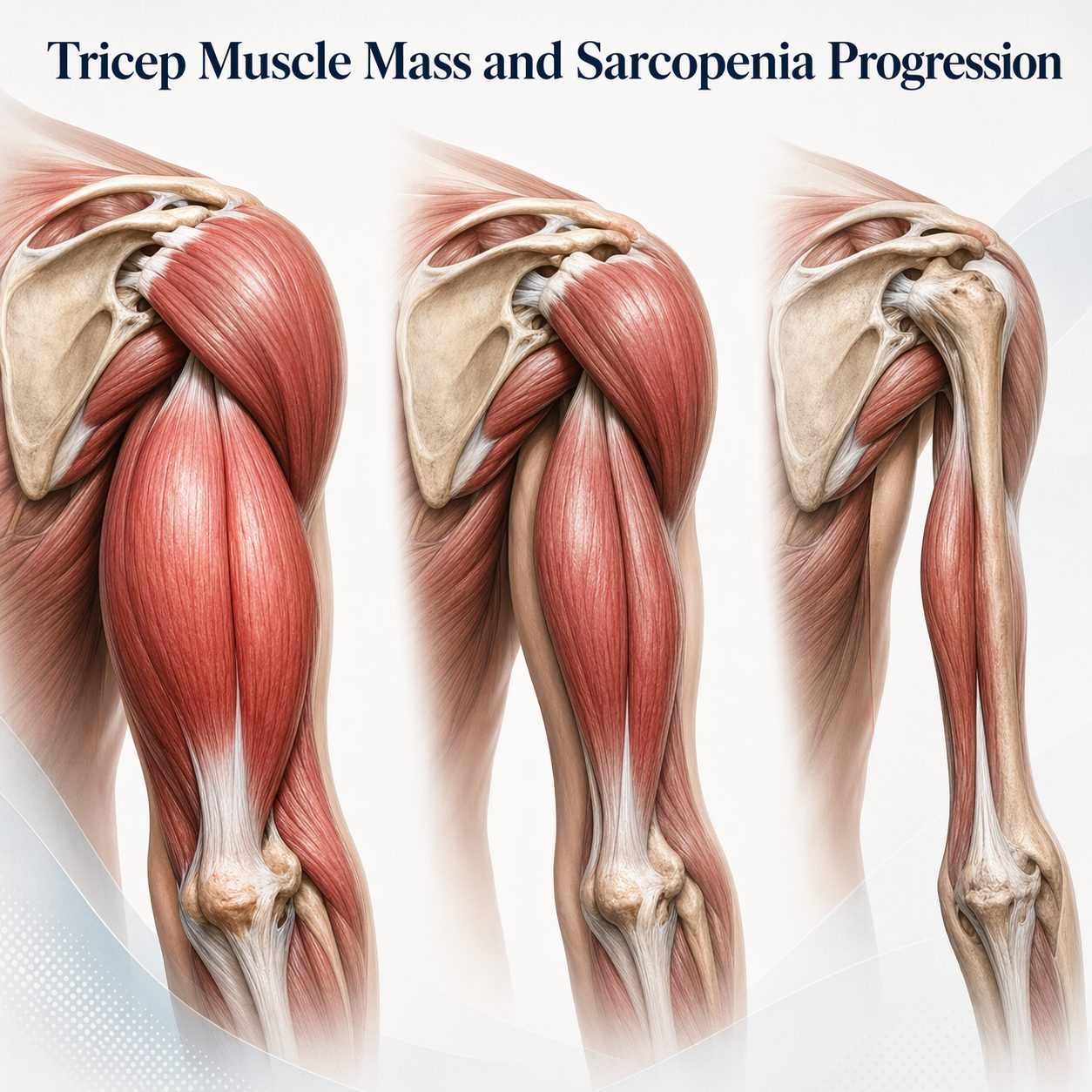
Sarcopenia — the progressive loss of muscle mass and function — begins as early as the fourth decade of life. Estimates suggest a loss of three to eight percent of muscle mass per decade, accelerating after age sixty. The tricep, as a large upper arm muscle, is a meaningful contributor to total lean mass. Its rate of decline serves as a useful marker of broader musculoskeletal deterioration.
The National Institute on Aging has funded extensive research confirming that upper limb muscle mass correlates strongly with overall sarcopenia severity. Individuals with faster upper body muscle loss show earlier onset of functional decline — defined as reduced capacity for tasks requiring sustained force, balance recovery, and fall prevention. For high-functioning professionals, these are direct determinants of physical independence across the lifespan.
Sarcopenia also carries metabolic consequences. Skeletal muscle is the primary site of insulin-stimulated glucose uptake, accounting for roughly eighty percent of post-meal glucose disposal. As tricep and broader muscle mass declines, insulin sensitivity falls, fasting glucose rises, and metabolic syndrome risk increases in a measurable pattern.
The Metabolic Role of Upper Body Muscle Tissue
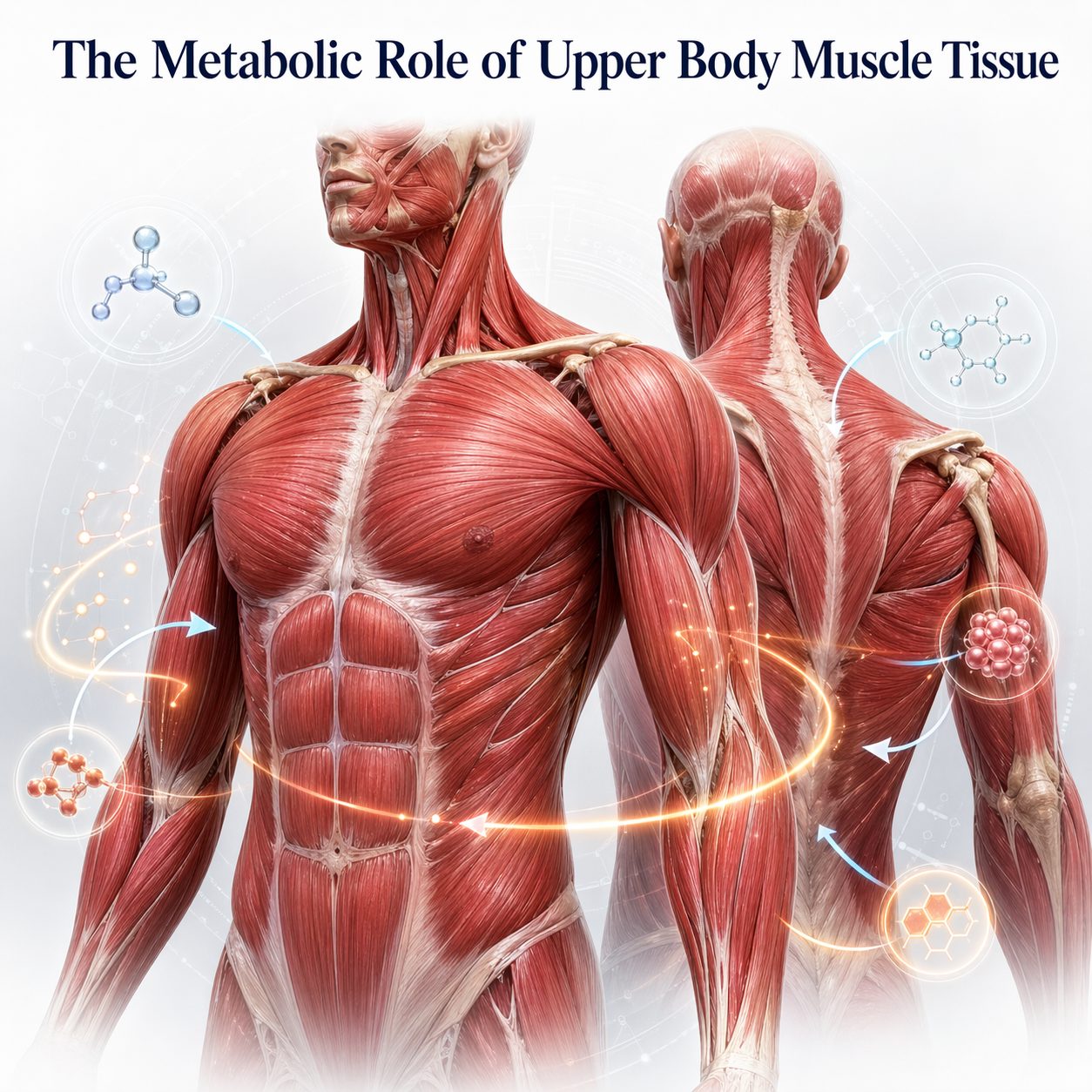
Skeletal muscle functions as a metabolically active signaling organ, releasing proteins called myokines during and after contraction. Among the most studied is irisin, which promotes fat burning, supports energy production at the cellular level, and has shown neuroprotective effects in emerging research. The tricep muscle, when trained consistently, contributes to this signaling output.
Muscle tissue also represents a significant share of the body's resting metabolic rate (RMR). Greater lean mass — including upper arm muscle — increases the calories the body burns at rest. For professionals managing body composition as a longevity variable, preserving tricep mass is a direct lever on metabolic efficiency and fat control.
Research from the American Diabetes Association consistently highlights upper extremity muscle mass as relevant to type 2 diabetes risk. Individuals with greater arm muscle mass relative to body weight show better blood sugar control, lower HbA1c trends, and reduced reliance on medication for glucose management over time.
Grip Strength, Tricep Integrity, and Longevity Biomarkers
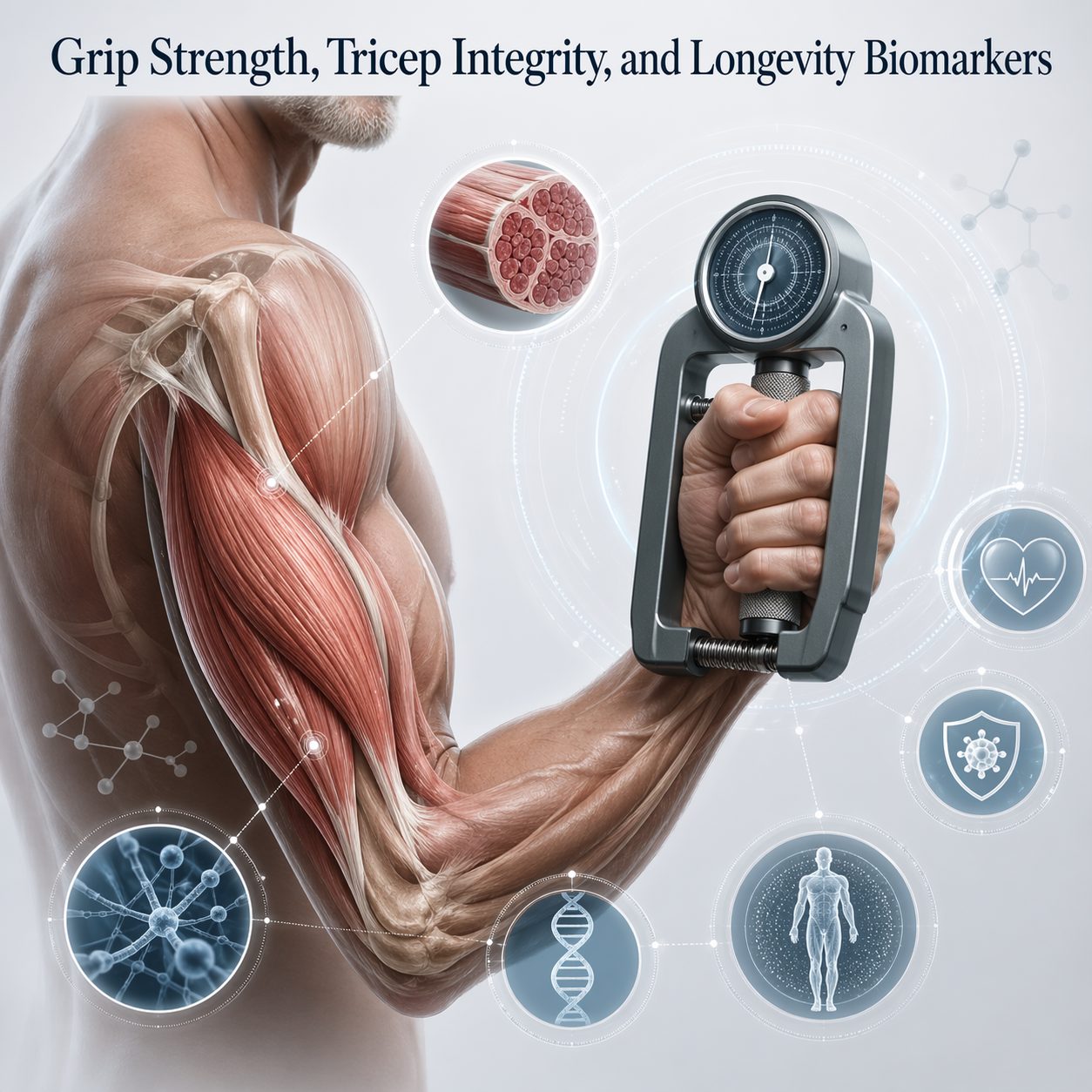
Grip strength has emerged as one of the most robust predictors of all-cause mortality in long-term research. Data from the UK Biobank — tracking over 500,000 participants — confirms that grip strength predicts cardiovascular death, cancer survival, and cognitive decline. These associations hold independently of age, sex, and physical activity level. While grip strength primarily reflects forearm and hand muscles, it links mechanistically to total upper arm integrity, including tricep condition.
The connection between tricep health and grip strength runs through shared neuromuscular pathways. Elbow extension force and grip production rely on overlapping motor control systems and similar fast-twitch muscle fiber reserves. Decline in one typically signals broader upper arm deterioration rather than isolated weakness.
For professionals using grip strength as a biological age proxy — a practice now common in executive health assessments — tricep conditioning is a modifiable upstream variable. Improving tricep mass and neuromuscular function can stabilize and often improve grip strength over time, with downstream effects on the broader longevity biomarker profile.
Hormonal Environment and Tricep Muscle Maintenance
Maintaining tricep mass becomes harder with age due to shifts in the hormonal environment. Testosterone, growth hormone, and insulin-like growth factor-1 (IGF-1) are the primary hormones driving muscle protein synthesis. All three decline with age. Testosterone begins a gradual reduction from the late twenties. The decline accelerates through the forties and fifties in both men and women.
This hormonal shift does not make tricep maintenance impossible — but it changes the stimulus required to preserve it. The muscle-building response to resistance training becomes less efficient with age. Research from the American College of Sports Medicine confirms that adults over forty require greater training intensity to achieve the same muscle growth seen in younger individuals. Adequate protein intake — particularly foods rich in the amino acid leucine — becomes increasingly relevant.
Cortisol — the primary stress hormone — exerts opposing pressure on muscle tissue. Chronically elevated cortisol, common among high-stress professionals, accelerates muscle breakdown and blunts the signals that support tricep maintenance. Managing cortisol through sleep, recovery, and stress reduction is directly relevant to preserving upper body muscle mass over time.
Tricep Function and Cardiovascular Health Correlations
The link between skeletal muscle mass and cardiovascular health is well-established. Research published in the Journal of the American Heart Association shows that low muscle mass independently predicts cardiovascular mortality. The mechanisms include elevated systemic inflammation, impaired autonomic regulation, and reduced cardiac output during exertion.
The tricep, as a contributor to total lean body mass, participates in this relationship. Greater upper body muscle mass links to lower resting heart rate, better baroreceptor sensitivity, and more favorable cholesterol profiles — including higher HDL and lower triglycerides. These associations persist after controlling for aerobic fitness. This suggests that resistance-trained muscle mass carries cardiovascular benefits beyond what VO2 max alone captures.
For the executive whose cardiovascular risk profile is actively monitored, tricep conditioning offers utility alongside aerobic training. It contributes to the composite physiological picture that shapes cardiovascular resilience through the fifth and sixth decades.
Tricep Tendon Health and Injury Risk in Sedentary Professionals
The tricep tendon — the attachment connecting muscle to the elbow — is a commonly overlooked injury site. Tendinopathy and partial tears carry significant functional consequences, particularly for professionals who engage in physically demanding recreation. These injuries develop through repetitive low-load strain, sudden high-force loading after deconditioning, and age-related changes in collagen structure and tendon flexibility.
Sedentary professionals who exercise infrequently but intensely face elevated tendon injury risk. The tricep tendon, weakened through extended disuse, is especially vulnerable to heavy pressing movements performed without adequate preparation. This pattern is well-documented in sports medicine and is increasingly common among middle-aged recreational athletes.
Tendon health responds well to consistent, progressive loading. Isometric and eccentric loading protocols have shown particular effectiveness in promoting collagen synthesis and structural tendon integrity. These approaches are clinically relevant for professionals returning to resistance training after extended breaks or managing early tendon discomfort.
READ ALSO: Latissimus Muscle Function and Grip Strength Decline in High-Performance Adults
Training Variables That Drive Tricep Adaptation
The tricep responds to resistance training through two primary pathways. The first is myofibrillar hypertrophy — growth in the size and number of contractile proteins within muscle fibers. The second is sarcoplasmic hypertrophy — an increase in the fluid and energy substrate volume within muscle cells. For longevity-oriented training, myofibrillar growth carries greater functional value. It directly increases force output and metabolic tissue density.
Elbow extension exercises — including overhead tricep extensions and close-grip pressing — load all three tricep heads. The long head receives the greatest activation in overhead positions due to its role at the shoulder. This makes overhead variations particularly valuable for complete tricep development. Both mechanical tension and metabolic stress drive muscle adaptation. Both require progressive resistance increases over time.
Training frequency matters as much as exercise selection. Research in the Journal of Strength and Conditioning Research supports training each muscle group two to three times per week for optimal growth in adults over forty. Single weekly sessions are insufficient to sustain a consistent muscle-building environment when anabolic efficiency declines with age.
READ ALSO: Protein Powder for Building Muscle: Your Aging Fitness Secret
Tricep Conditioning and Biological Age Assessment

Biological age assessments increasingly include lean muscle mass and upper extremity strength as component variables. DEXA scanning (dual-energy X-ray absorptiometry) can measure regional muscle mass directly, including upper arm composition. This provides a baseline against which change can be tracked over time. Tricep mass is visible within upper arm lean mass data from a standard DEXA report.
Bioelectrical impedance analysis (BIA) offers a more accessible — though less precise — option for monitoring lean mass trends. When used consistently under controlled conditions, BIA can detect meaningful shifts in upper body composition. For professionals tracking health metrics between full DEXA assessments, serial BIA measurements offer a practical monitoring tool.
Combining tricep-specific performance measures — such as elbow extension force or overhead pressing capacity relative to body weight — with body composition data creates a more complete picture of upper body biological age. Strength-to-mass ratios are more informative than raw mass figures alone. They capture neuromuscular efficiency alongside structural tissue volume.
READ ALSO: Leg Muscle Strength for Balanced Energy
Evidence-Based Options for the Informed Professional
The evidence on tricep health and longevity points toward a clear set of options for professionals who want to engage with this variable precisely. Incorporating elbow extension movements two to three times per week — with progressive load increases — provides the stimulus needed for muscle adaptation in middle-aged adults. Ensuring adequate dietary protein with sufficient leucine content supports muscle building in the context of age-related hormonal decline. DEXA scanning establishes the most accurate regional lean mass baseline for longitudinal tracking. Managing cortisol through sleep quality and structured recovery reduces the catabolic pressure on muscle tissue. Consulting a clinician with sports medicine or musculoskeletal expertise can support programming decisions that account for tendon health, training history, and the specific hormonal variables relevant to the professional's age and health profile.
UP NEXT: The Structural Case for Posterior Chain Development: Back Muscle Function, Posture, and Longevity Performance
How This Affects Your Biological Age
Declining tricep muscle mass is a measurable marker of sarcopenia progression, and adults who lose significant upper arm lean mass between the ages of forty and sixty show grip strength trajectories and metabolic profiles consistent with a biological age three to five years older than their chronological age. WholeLiving's Biological Age Estimation Model incorporates this factor directly — your assessment takes under five minutes.
Ready to understand how these factors are influencing your biological age right now? [Take the Biological Age Assessment →]







