Skin biological age is a measurable and increasingly monitored variable in the performance longevity space — and for executives in the 35-to-60 demographic, the rate of dermal collagen degradation is a direct marker of systemic oxidative stress and cellular aging. Topical ascorbic acid, when formulated at clinically effective concentrations and stable delivery systems, intervenes in that process at the biochemical level — stimulating collagen synthesis, neutralizing reactive oxygen species, and attenuating UV-induced DNA damage in dermal tissue. For high-performing professionals who monitor biological age across multiple systems, skin is not a vanity variable. It is a tissue-level readout of the same oxidative and inflammatory processes driving systemic aging.
What Makes a Vitamin C Serum Clinically Effective

Not all vitamin C serums deliver equivalent biological outcomes. The difference between a clinically effective formulation and a cosmetically marketed one lies in three variables: the form of ascorbic acid used, its concentration, and the stability of the delivery system. Each variable determines whether the active compound reaches the dermis at a sufficient concentration to drive measurable collagen synthesis and oxidative stress reduction. Without all three in place, the compound degrades before it can exert any meaningful biological effect.
L-ascorbic acid is the only form of vitamin C with direct, well-documented evidence for dermal collagen stimulation and antioxidant activity in skin tissue. Derivative forms — including ascorbyl glucoside, magnesium ascorbyl phosphate, and ascorbyl palmitate — require enzymatic conversion to L-ascorbic acid before they become biologically active. That conversion is variable and often incomplete. For professionals seeking measurable outcomes rather than marketing claims, L-ascorbic acid in a stabilized formulation remains the benchmark form.
Concentration also determines clinical outcome. Research published in the Journal of Investigative Dermatology has established that L-ascorbic acid must reach a threshold concentration in dermal tissue to produce meaningful collagen stimulation. Formulations below that threshold produce cosmetic rather than clinical effects. Beyond a certain point, higher concentrations do not produce proportionally greater outcomes. They may also increase skin irritation without adding benefit. The clinically relevant range is well established in the research literature, and the best vitamin C serum formulations are built around it.
The Biochemistry of Ascorbic Acid in Dermal Tissue
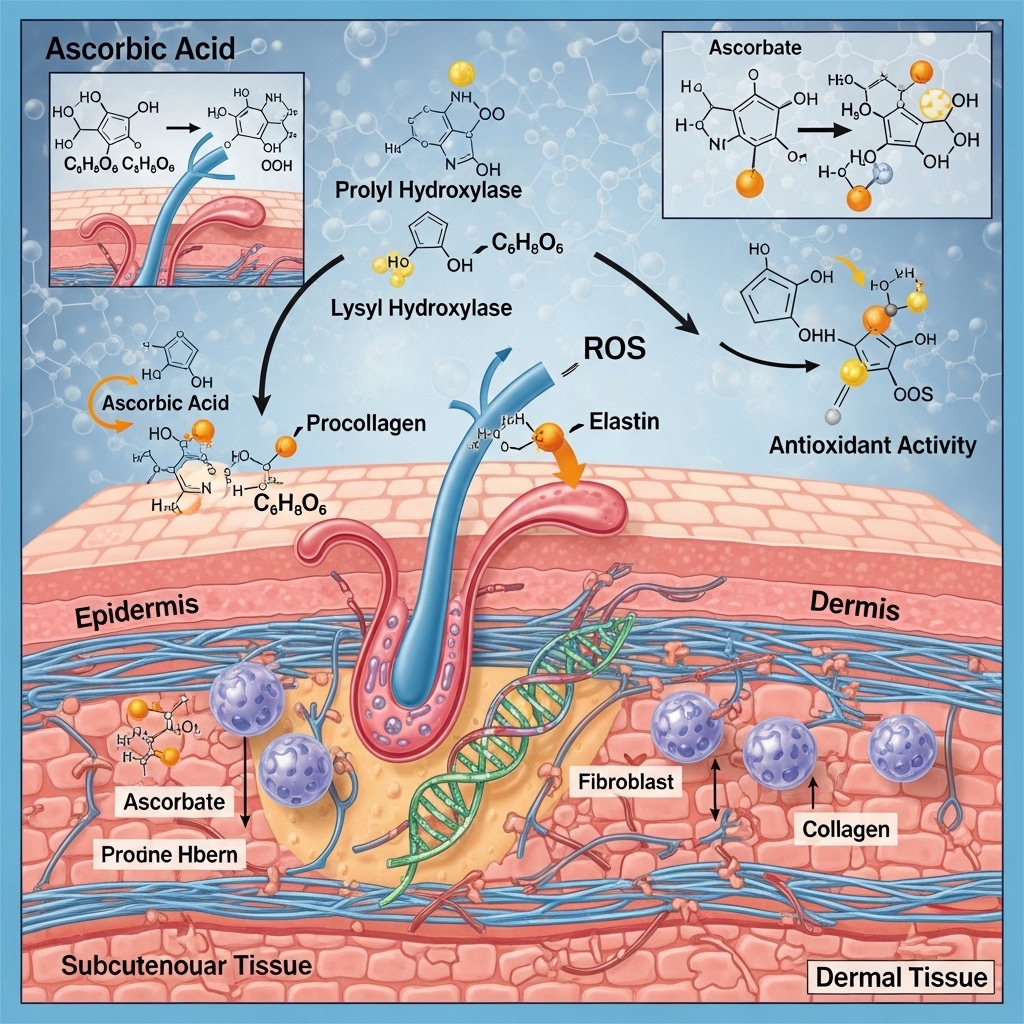
Understanding how vitamin C functions in dermal tissue clarifies why formulation quality matters so much. L-ascorbic acid serves two primary biochemical roles in skin. First, it acts as a cofactor in collagen synthesis. Second, it functions as a direct antioxidant that neutralizes reactive oxygen species generated by UV exposure, pollution, and metabolic processes. Both roles are relevant to the biological aging of skin tissue — and both are concentration-dependent.
In collagen synthesis, ascorbic acid acts as a required cofactor for the enzymes prolyl hydroxylase and lysyl hydroxylase. These enzymes stabilize the triple-helix structure of collagen molecules. Without adequate ascorbic acid, collagen production continues but produces structurally unstable collagen that degrades more rapidly. In the context of dermal aging — where collagen density declines measurably from the mid-thirties onward — this cofactor role is directly relevant to skin biological age.
As an antioxidant, L-ascorbic acid neutralizes free radicals before they can damage collagen fibers, elastin, and cell membrane lipids. UV radiation generates reactive oxygen species in the dermis continuously. In the absence of adequate antioxidant buffering, this oxidative damage accumulates as cross-linked collagen, elastin fragmentation, and melanin dysregulation. The best vitamin C serum formulations address both the synthetic and the protective role of ascorbic acid simultaneously. This is why they consistently outperform formulations that rely on derivative forms with incomplete conversion rates.
pH, Stability, and the Formulation Variables That Determine Outcomes
The efficacy of any vitamin C serum depends critically on its formulation chemistry — specifically its pH and its stability over time. L-ascorbic acid is inherently unstable. It oxidizes rapidly when exposed to air, light, and water. It converts first to dehydroascorbic acid and then to diketogulonic acid — a form with no biological activity in the skin. A serum that has undergone significant oxidation before application delivers little to no clinical benefit, regardless of its original concentration.
Effective formulations address this instability through two primary strategies. First, they formulate at a low pH — typically between 2.5 and 3.5. This maintains the ascorbic acid molecule in its reduced, biologically active form. It also supports dermal penetration by keeping the compound in its uncharged, lipid-compatible state. Second, they use packaging that limits air and light exposure — opaque, airtight containers that reduce oxidative degradation between uses. These are not cosmetic packaging choices. They are biochemical requirements for maintaining product efficacy through its shelf life.
The best vitamin C serum formulations also frequently incorporate antioxidant synergists — most commonly vitamin E and ferulic acid. These stabilize the ascorbic acid molecule and extend its antioxidant activity in the skin. Research from Duke University, examining the combination of L-ascorbic acid, vitamin E, and ferulic acid, found that this combination produced significantly greater photoprotective effects than any single antioxidant alone. This synergistic formulation approach is now considered a benchmark in evidence-based topical antioxidant therapy.
Collagen Synthesis, Dermal Density, and Skin Biological Age
Collagen density in the dermis declines at a measurable rate from the mid-thirties onward. Under normal aging conditions, the decline runs at approximately one percent per year. Chronic UV exposure, oxidative stress, and systemic inflammation accelerate that rate significantly. For executives in the 35-to-60 demographic who monitor biological age across multiple tissue systems, dermal collagen density is an increasingly accessible and relevant tissue-level marker.
The relationship between topical ascorbic acid and collagen synthesis is well established in the research literature. Studies examining split-face designs — where one side of the face receives active treatment and the other serves as a control — have documented measurable increases in collagen density, collagen fiber organization, and dermal thickness. These changes follow consistent topical ascorbic acid application over a period of weeks to months. These are not subjective improvements in appearance. They are measurable structural changes in tissue composition.
For high-performing professionals, the significance of this evidence extends beyond aesthetic outcomes. Dermal collagen density reflects the same systemic oxidative and inflammatory environment that drives collagen degradation in vascular tissue, joint cartilage, and other connective tissue systems throughout the body. Skin is accessible and visible. This makes it a useful proxy tissue for monitoring the oxidative stress burden that affects aging across multiple organ systems simultaneously. The best vitamin C serum addresses the dermal expression of that burden directly.
Photoprotection, UV Damage, and Oxidative Stress Accumulation
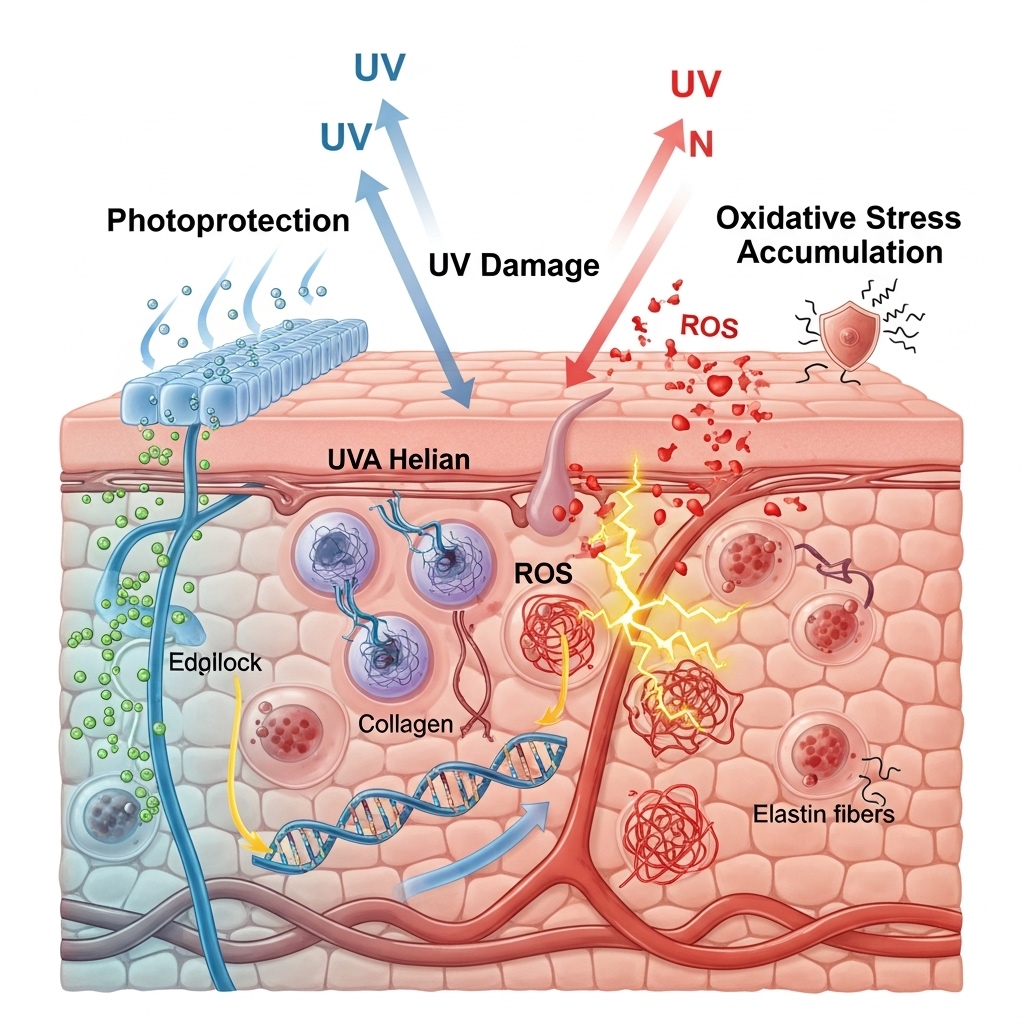
UV radiation is the single largest environmental driver of accelerated skin biological aging. It is responsible for what researchers term photoaging — a process distinct from and additive to intrinsic chronological aging. UV exposure generates reactive oxygen species in the dermis. These damage DNA, degrade collagen and elastin, and disrupt melanocyte regulation. Over decades, this oxidative damage accumulates as reduced collagen density, increased cross-linking of collagen fibers, elastin fragmentation, and uneven pigmentation.
Topical antioxidant therapy — specifically the application of a stabilized L-ascorbic acid serum — addresses UV-induced oxidative damage through two mechanisms. First, it neutralizes reactive oxygen species generated by UV exposure before they can damage dermal structures. Second, it partially inhibits the UV-induced upregulation of matrix metalloproteinases — the enzymes responsible for collagen degradation. This reduces the net rate of collagen loss following sun exposure. Both mechanisms are documented in peer-reviewed research and represent the primary evidence base for ascorbic acid as a photoprotective topical agent.
Topical vitamin C is not a substitute for broad-spectrum UV protection. It functions as a complementary layer of photoprotective defense — not a replacement for physical sunscreen. The best vitamin C serum protocols incorporate both. They leverage the documented synergy between topical antioxidant application and UV-filtering agents to produce a more complete photoprotective strategy than either approach achieves alone.
Hyperpigmentation, Melanin Regulation, and Even Skin Tone

Hyperpigmentation — the uneven accumulation of melanin in the dermis resulting from UV exposure, hormonal shifts, and post-inflammatory responses — is among the most common skin biological aging markers in the 35-to-60 demographic. It is also one of the most responsive to topical ascorbic acid intervention. L-ascorbic acid inhibits tyrosinase — the rate-limiting enzyme in melanin synthesis. This reduces the overproduction of melanin that underlies uneven skin tone, age spots, and post-inflammatory hyperpigmentation.
This mechanism of action is distinct from the exfoliating or bleaching approaches used by other topical brightening agents. Rather than removing existing pigmentation through chemical exfoliation, ascorbic acid reduces the rate of new melanin production at the enzymatic level. The result, with consistent application over several weeks, is a gradual and progressive evening of skin tone. For professionals whose skin reflects years of UV exposure and high-stress cortisol burden, this mechanism addresses one of the most visible markers of skin biological age directly.
Cortisol elevation — chronic in the executive demographic — also contributes to hyperpigmentation through its stimulating effect on melanocyte-stimulating hormone pathways. For professionals managing high allostatic load, topical ascorbic acid intervention addresses the dermal consequence of that cortisol burden at the tissue level. This does not replace systemic stress management. However, it represents a targeted, evidence-supported intervention for one of its visible dermal outcomes.
Inflammatory Markers, Systemic Oxidative Stress, and Skin Health
The skin does not age in isolation. Its biological aging rate reflects the systemic inflammatory and oxidative environment in which it operates. Elevated inflammatory markers — including hs-CRP and interleukin-6 — accelerate collagen degradation, impair wound healing, and promote the enzyme activity that breaks down dermal structure. For executives who monitor systemic inflammatory markers as part of a performance health protocol, skin biological age is a useful additional data point in that broader picture.
Research from the National Institutes of Health and associated research bodies has examined the relationship between systemic oxidative stress and accelerated skin aging. The consistent finding is that skin biological age — measured through collagen density, elastin integrity, and epidermal function — tracks closely with systemic markers of oxidative burden and inflammation. This means that topical interventions, while directly relevant to dermal outcomes, operate within a broader systemic context that topical application alone cannot fully address.
The best vitamin C serum therefore functions most effectively as part of a layered approach. It works alongside strategies that address systemic oxidative stress — through dietary antioxidant intake, sleep quality, and inflammatory marker management — while using topical ascorbic acid to intervene directly at the dermal level. Professionals who approach skin biological age as a tissue-level expression of systemic aging will extract the most clinically meaningful value from their topical protocol.
Selecting the Best Vitamin C Serum: What the Evidence Supports

The evidence base for topical ascorbic acid supports a clear set of selection criteria for professionals seeking clinical rather than cosmetic outcomes. Formulation form matters first. L-ascorbic acid is the benchmark. Derivative forms carry insufficient conversion evidence to support equivalence claims. Concentration places second — the clinically relevant range is well documented, and formulations outside it are unlikely to produce measurable collagen or antioxidant outcomes.
Stability infrastructure places third. Packaging that limits air and light exposure is a biochemical requirement, not a cosmetic preference. Beyond these primary criteria, the presence of synergistic antioxidant co-factors — specifically vitamin E and ferulic acid — is supported by Duke University research. That research demonstrated significantly enhanced photoprotective and antioxidant efficacy compared to L-ascorbic acid alone. Formulations that include this combination represent the current evidence benchmark for topical antioxidant therapy.
Additional formulation variables — including niacinamide for complementary melanin regulation, hyaluronic acid for dermal hydration support, and peptide complexes for collagen stimulation — are supported by varying degrees of evidence. These additions do not replace the primary ascorbic acid mechanism. However, they may contribute complementary benefits within a well-formulated product. The best vitamin C serum for a clinically oriented protocol incorporates these variables based on evidence rather than marketing.
READ ALSO: Anti Aging and Skin Care: Restorative Tips for Your Glow
Application Protocol and the Conditions for Efficacy
A clinically effective vitamin C serum requires consistent, protocol-driven application to produce measurable outcomes. Inconsistent use — applying the serum sporadically or discontinuing during periods of travel or schedule disruption — undermines the cumulative collagen stimulation and antioxidant loading that drives clinical results. The dermal outcomes documented in research are products of consistent daily application over weeks to months. They are not products of episodic use.
Morning application is supported by the evidence base as the optimal timing for topical antioxidant therapy. Applied before UV exposure, a stabilized L-ascorbic acid serum loads the dermis with antioxidant capacity. That capacity is then available to neutralize reactive oxygen species generated throughout the day. This timing maximizes the photoprotective function of the serum and aligns with the skin's natural antioxidant depletion pattern following sun exposure. Evening application does not produce equivalent photoprotective benefit. It may, however, contribute to the collagen synthesis and tissue repair processes that are more active during overnight recovery.
Storage conditions also affect product efficacy in ways that many protocols overlook. Oxidative degradation of L-ascorbic acid accelerates significantly with heat and light exposure. Storing the serum in a cool, dark environment maintains formulation integrity through the product's use period. Monitoring the product for color changes that indicate oxidation is also a reliable quality check. A serum that has shifted from clear or pale yellow to orange or brown has undergone significant oxidative degradation. It is unlikely to deliver its labeled clinical benefits regardless of its original formulation quality.
READ ALSO: Dry Skin Moisturizer Tips for Soft, Nourished Skin
Skin Biological Age as a Longevity Monitoring Variable
The framing of skin health as a vanity concern rather than a biological aging variable has historically kept it at the margins of performance health protocols. That framing is increasingly inconsistent with the evidence. Skin biological age is a legitimate tissue-level marker of the systemic oxidative and inflammatory processes that drive aging across all organ systems. It is measurable through collagen density assessment, transepidermal water loss, elasticity testing, and epidermal turnover rate.
For executives who already monitor biological age through epigenetic clocks, cardiovascular biomarkers, and metabolic panels, adding skin biological age assessment provides a tissue-level readout that is accessible, non-invasive, and highly responsive to intervention. Changes in skin biological age often reflect changes in the systemic oxidative and inflammatory environment. Notably, these changes frequently appear before they show up in blood-based biomarkers. This responsiveness makes skin a useful early-signal tissue for monitoring the effects of protocol adjustments across the broader health system.
The best vitamin C serum, applied consistently within a broader performance health protocol, contributes to skin biological age management at the tissue level. It also reflects the systemic antioxidant and anti-inflammatory environment the professional maintains through their overall health architecture. Treated as a clinical intervention rather than a cosmetic product, topical ascorbic acid earns its place in the evidence-based performance longevity protocol.
READ ALSO: Anti-Aging and Skin Care Tips for Timeless Beauty
Building an Evidence-Based Topical Antioxidant Protocol
Professionals who seek to address skin biological age through the evidence base have a clear set of options available. Selecting a stabilized L-ascorbic acid formulation at a clinically relevant concentration — combined with vitamin E and ferulic acid synergists — represents the current benchmark supported by research. Establishing a consistent morning application protocol maximizes photoprotective loading and aligns with the skin's antioxidant depletion pattern.
Storing the product in conditions that limit oxidative degradation maintains formulation integrity through its use period. Integrating skin biological age assessment into a broader biological age monitoring protocol — alongside epigenetic, cardiovascular, and metabolic variables — positions topical antioxidant therapy within its appropriate clinical context.
Addressing the systemic oxidative and inflammatory environment through sleep quality, dietary antioxidant intake, and inflammatory marker management ensures that topical intervention operates within a supportive systemic framework. The best vitamin C serum delivers its most meaningful clinical outcomes when it functions as one layer of a coherent, evidence-driven performance health protocol — not as a standalone cosmetic product.
UP NEXT: Korean Skin Care Secrets for Glowing, Healthy Skin
How This Affects Your Biological Age
Consistent use of a clinically formulated vitamin C serum — one that stabilizes dermal collagen synthesis and neutralizes UV-induced oxidative stress — directly addresses two of the primary tissue-level drivers of accelerated skin biological aging, with research linking chronic oxidative burden and collagen degradation to measurable increases in biological age that extend beyond the skin to systemic aging markers. WholeLiving's Biological Age Estimation Model incorporates this factor directly — your assessment takes under five minutes.
Ready to understand how these factors are influencing your biological age right now? [Take the Biological Age Assessment →]