Persistent lower abdominal pain is not a symptom to defer until the next quarterly physical. For executives operating under sustained cognitive and physiological load, unresolved visceral pain frequently signals underlying dysfunction — including pelvic floor dyssynergia, chronic low-grade intestinal inflammation, or early-stage genitourinary pathology — each capable of elevating systemic inflammatory markers such as CRP and IL-6, which are independently associated with accelerated biological aging and diminished executive cognitive function. Dismissing this signal as stress-related or situational delays diagnosis and compounds downstream health costs, including compromised sleep architecture, cortisol dysregulation, and reduced physical performance capacity.
Pain on Lower Abdomen: Why Anatomical Location Drives Diagnosis
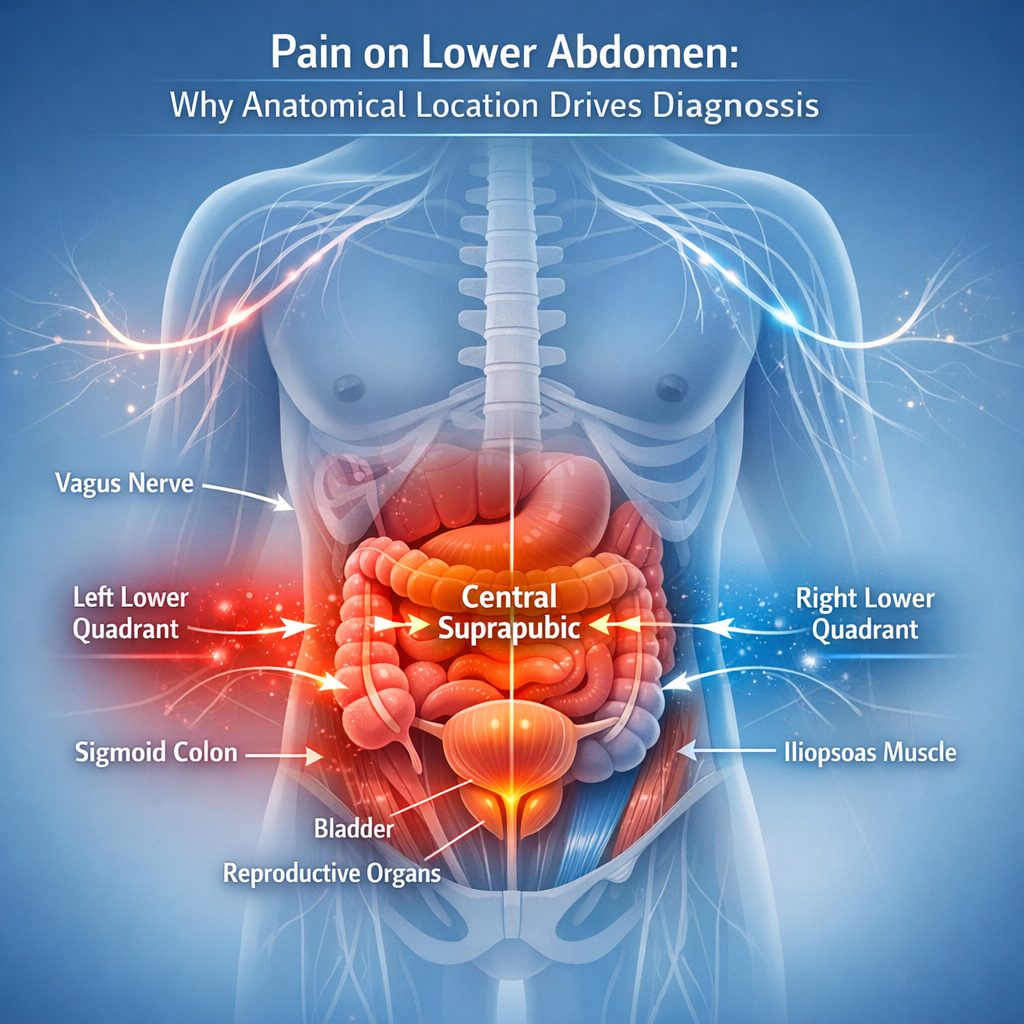
The lower abdomen is not a single anatomical structure. Instead, it is a densely populated region. It houses the sigmoid colon, bladder, ureters, reproductive organs, lymph nodes, and segments of the iliopsoas muscle complex. When pain on lower abdomen presents, its precise quadrant, character, and timing carry significant diagnostic weight. For example, left lower quadrant pain behaves differently from right-sided or central suprapubic pain. Conflating these distinctions delays accurate diagnosis by months in many cases.
Clinicians use a quadrant-based localization framework because referred pain is common in visceral pathology. In referred pain, the source of the signal is anatomically distant from where the patient feels it. The vagus nerve and spinal afferent pathways create overlapping sensory maps that frequently mislead both patient and clinician. Consequently, a professional who attributes intermittent lower abdominal cramping to stress or diet may be missing a progressing underlying condition entirely.
A 2020 review in the American Journal of Gastroenterology found that functional lower gastrointestinal disorders are frequently underdiagnosed in high-functioning adults. Notably, these adults tend to normalize symptoms as occupational stress responses. As a result, clinical underreporting in this demographic extends diagnostic timelines by an average of four years. That delay compounds consequences significantly when inflammatory or structural pathology is the actual driver.
Gastrointestinal Causes of Pain on Lower Abdomen That Carry Systemic Risk
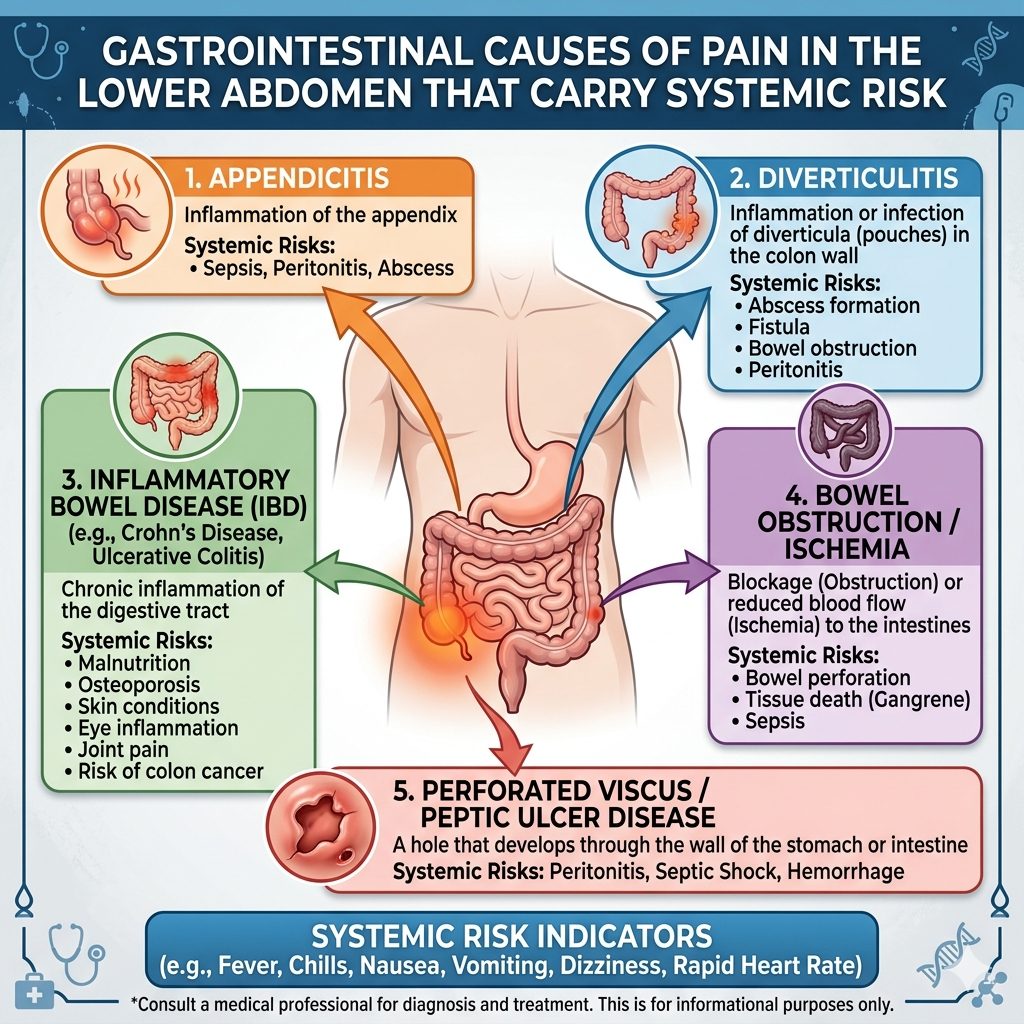
Diverticular disease is one of the most consequential and overlooked causes of recurrent left lower abdominal pain in adults over 40. Diverticulosis — the presence of small pouches in the colonic wall — is largely silent until inflammation or rupture occurs. At that point, systemic inflammatory burden escalates sharply. Furthermore, elevated CRP and white cell count in acute diverticulitis are not isolated events. They signal a gut lining under sustained pressure.
Inflammatory bowel disease — including Crohn's disease and ulcerative colitis — can present with pain on lower abdomen as a primary symptom. Additionally, fatigue often accompanies it and gets mistaken for overwork or poor sleep. Research through the NIH's National Institute of Diabetes and Digestive and Kidney Diseases links the systemic inflammatory load from active IBD to accelerated telomere shortening. Telomere length is a direct, measurable marker of biological aging. For executives already managing high cortisol environments, untreated gut inflammation compounds biological age in ways that routine bloodwork rarely captures.
Colorectal pathology — including polyps and early-stage malignancy — must also stay in the differential for any adult over 40 with persistent lower abdominal symptoms. This is especially true when bowel habits change or unexplained weight loss occurs. Moreover, the American Cancer Society moved the recommended colorectal screening age to 45. That threshold directly overlaps with the WholeLiving core demographic. Therefore, treating intermittent lower abdominal discomfort as purely functional — without investigation — carries measurable mortality risk.
Genitourinary Pathology and Pain on Lower Abdomen: The Diagnostic Blind Spot
In male professionals, pain on lower abdomen frequently connects to genitourinary pathology without classic urological symptoms. Chronic prostatitis and pelvic floor dysfunction generate suprapubic and perineal pain. That pain often radiates into the lower abdomen. The NIH classifies chronic pelvic pain syndrome as a distinct clinical entity. It carries independent impact on sleep architecture, quality of life, and psychological resilience.
In female professionals, endometriosis remains one of the most underdiagnosed conditions generating chronic pain on lower abdomen. Research in Human Reproduction Update found that the average diagnostic delay for endometriosis in high-income countries runs between six and ten years. During that window, inflammatory burden increases, adhesions form, and ovarian reserve declines without intervention. Consequently, women in leadership roles who normalize cyclical or persistent pelvic pain pay a measurable long-term physiological cost.
Similarly, urinary tract pathology — including recurrent cystitis and bladder dysfunction — generates lower abdominal pain that professionals frequently self-treat or defer. Recurrent urinary tract infections drive up systemic inflammatory cytokines, including IL-6. The Harvard T.H. Chan School of Public Health has linked IL-6 elevation in multiple studies to higher cardiovascular risk, cognitive decline, and reduced physical output in middle-aged adults. In other words, the chain between a localized genitourinary symptom and systemic performance loss is mechanistically established — not theoretical.
Musculoskeletal Drivers of Pain on Lower Abdomen

Pain on lower abdomen does not always come from visceral structures. The iliopsoas, rectus abdominis, and obturator internus muscles — along with the pelvic floor fascia — generate somatic pain that closely mimics visceral pathology. In fact, executives with sedentary schedules, high travel frequency, and compressed recovery windows appear disproportionately among patients with musculoskeletal lower abdominal pain.
Pelvic floor dysfunction — whether overactive or underactive — produces lower abdominal pressure, urinary urgency, and lumbar discomfort. Moreover, physical medicine research consistently identifies sitting for more than eight hours per day as a primary driver of pelvic floor coordination problems in otherwise high-functioning adults. As a result, the occupational posture most associated with executive productivity simultaneously degrades the muscular infrastructure supporting core stability and visceral function.
In addition, inguinal and femoral hernias are mechanical causes of lower abdominal and groin pain that high-performing professionals frequently defer. However, when left unrepaired — particularly when tissue becomes trapped — the outcome escalates from elective to emergency surgery. That is an avoidable outcome with significant recovery implications for any professional whose schedule cannot absorb unplanned surgical convalescence.
Inflammatory Markers, Biological Age, and Unresolved Pain on Lower Abdomen
Persistent lower abdominal pain that goes unevaluated represents an ongoing inflammatory signal. The body's pain signaling and immune systems are not siloed. Sustained visceral input activates central sensitization pathways and promotes low-grade systemic inflammation well beyond the symptomatic region. Furthermore, this mechanism is especially consequential for adults aged 35 to 60, where inflammatory burden is one of the most reliable predictors of faster biological aging.
CRP, IL-6, and TNF-alpha — three inflammatory markers measurable through advanced blood panels — rise across multiple lower abdominal conditions, including IBD, chronic prostatitis, endometriosis, and recurrent urinary tract infections. Notably, the Framingham Heart Study identified elevated CRP as an independent predictor of cardiovascular events, cognitive decline, and all-cause mortality across multiple decades of follow-up. Therefore, a lower abdominal symptom that drives chronic CRP elevation is a systemic risk factor — not a localized complaint.
Sleep is another performance variable that unresolved lower abdominal pathology directly affects. Pain of any origin — visceral, muscular, or inflammatory — disrupts slow-wave sleep and REM continuity. As a result, physiological recovery suffers, and next-day cognitive output, hormonal regulation, and immune function all decline. For executives tracking HRV and sleep quality through wearable devices, persistent lower abdominal discomfort is a measurable drag on the systems that executive function depends on.
READ ALSO: Diarrhea After Eating: Gentle Ways to Support Digestion
Cortisol, the Gut-Brain Axis, and Lower Abdominal Symptoms
High-performing professionals operate in sustained high-stress environments. The gut-brain axis translates that physiological state directly into digestive function. Cortisol and corticotropin-releasing hormone alter gut wall permeability, speed up colonic transit, and lower visceral pain thresholds. Consequently, pain on lower abdomen often intensifies during periods of high occupational demand. What professionals label as stress-related gut discomfort frequently reflects cortisol-driven disruption layered over existing structural or inflammatory pathology.
Research in psychoneuroimmunology shows that the enteric nervous system — housing more than 100 million neurons — responds to stress-axis activation in ways that worsen existing visceral pathology. For a professional with subclinical diverticular disease or an overactive pelvic floor, sustained cortisol elevation does not create the underlying problem. However, it reliably worsens symptom intensity and obscures the clinical pattern that would otherwise prompt earlier evaluation.
Furthermore, the gut-brain axis runs in both directions. Unresolved gastrointestinal pain generates upward signaling that affects mood, cognitive bandwidth, and decision-making quality. The vagal pathway carries visceral pain signals that activate brain structures involved in threat appraisal and executive function. Therefore, chronic lower abdominal discomfort is not neurologically neutral — it actively draws on cognitive resources that professionals in high-stakes roles cannot afford to redirect toward pain processing.
READ ALSO: Liver Cleansing Detox to Clear Out What Drains You
Diagnostic Evaluation: What a Rigorous Workup Covers
A thorough evaluation of pain on lower abdomen goes beyond single-organ assessment. The range of possible causes is wide enough to require a stepwise approach. That approach begins with history, physical examination, and targeted laboratory work — before imaging enters the picture. A complete blood count, CRP, erythrocyte sedimentation rate, urinalysis, and stool calprotectin provide an initial inflammatory and infectious profile. Together, these results guide the next diagnostic layer.
Imaging selection follows clinical suspicion. Ultrasound offers accessible, radiation-free assessment of pelvic and abdominal structures. It serves as the appropriate first-line modality for most lower abdominal presentations. In contrast, CT imaging with contrast addresses suspected acute pathology — including diverticulitis with abscess or blocked urinary drainage. Additionally, MRI remains the gold standard for soft tissue assessment, including endometriosis staging, pelvic floor mapping, and sacral nerve pathology.
Colonoscopy is indicated in any adult over 45 with lower abdominal symptoms that less invasive workup has not fully explained. This is especially true in the presence of altered bowel habit, rectal bleeding, or family history of colorectal malignancy. Nevertheless, many professionals defer this investigation because scheduling is inconvenient or the preparation disruptive. That deferral is a risk calculation the evidence does not support for this demographic.
READ ALSO: Gut Cleanse Tips for a Happier Stomach
When Functional Diagnoses Apply to Pain on Lower Abdomen
When structural pathology has been excluded through appropriate investigation, functional gastrointestinal disorders — including irritable bowel syndrome — represent a clinically legitimate and well-understood diagnosis. The Rome IV criteria provide a validated diagnostic framework that gastroenterological bodies accept internationally. In other words, a functional diagnosis is not a default category for unexplained pain.
However, a functional diagnosis does not mean symptoms are unreal or inconsequential. IBS links to altered gut microbiome composition, increased gut wall permeability, and heightened visceral sensitivity. All three carry downstream effects on immune function and inflammatory marker profiles. As a result, a professional who receives a functional diagnosis and treats the matter as resolved — without addressing these underlying mechanisms — misses a significant part of the clinical picture.
Evidence-based treatments for functional lower abdominal pain include low-FODMAP dietary protocols, which peer-reviewed trials support. Additionally, cognitive behavioral therapy adapted for chronic pain, gut-directed hypnotherapy, and strain-specific probiotic supplementation all carry evidence support. These are first-line treatments backed by gastroenterological society guidelines — not speculative add-ons.
Pelvic Floor Assessment as an Overlooked Diagnostic Step
Pelvic floor dysfunction generates a symptom cluster that includes lower abdominal pressure, urinary urgency, and lumbar discomfort. Clinicians outside urogynecology and physical medicine frequently underscreen for this condition in professional populations. Yet the presentation is common, measurable, and treatable through specialist physical therapy with a strong evidence base.
Assessment by a pelvic floor physiotherapist covers both external and internal evaluation of muscle tone, coordination, and endurance. This process identifies overactive patterns — where muscles stay in chronic contraction — as well as underactive patterns, where reduced activation contributes to instability and referred abdominal pain. Furthermore, neither pattern resolves through general core conditioning or rest alone.
For male professionals in particular, pelvic floor dysfunction remains underrecognized as a driver of chronic pelvic and lower abdominal pain. Referrals from urology and primary care to pelvic floor physiotherapy in men stay low relative to prevalence data. Consequently, integrating pelvic floor assessment into a comprehensive evaluation of recurrent lower abdominal symptoms closes a diagnostic gap that standard workups consistently leave open.
Integrating Evidence Into a High-Performance Health Protocol

The evidence across gastrointestinal, genitourinary, musculoskeletal, and stress physiology research points to a consistent conclusion. Pain on lower abdomen that persists beyond two to four weeks, recurs in a pattern, or accompanies systemic symptoms warrants formal medical evaluation. Self-monitoring, dietary self-experimentation, and waiting for workload to decrease are not evidence-supported responses in this demographic. Moreover, the diagnostic window for structural pathology is often narrow. Deferring evaluation consistently converts manageable conditions into complex ones.
A performance-focused health strategy for professionals in this age range includes baseline inflammatory biomarker panels — CRP, IL-6, and calprotectin — as part of annual or biannual preventive assessment. Additionally, imaging and endoscopic screening calibrated to age and risk profile belong in the same preventive framework. Pelvic floor assessment with a specialist in physical medicine or urogynecology is an underused but evidence-supported evaluation pathway. It is particularly relevant for professionals with recurrent lower abdominal or pelvic symptoms that standard workup does not fully explain.
The optimization frameworks that high-performing professionals apply to sleep, cognitive performance, and metabolic health extend — without exception — to gastrointestinal and pelvic health. The inflammatory load, cortisol disruption, and sleep damage generated by unresolved pain on lower abdomen act on the same biological systems that performance protocols protect. Therefore, resolving the source of that pain is not a secondary health priority. It is a prerequisite for the physiological environment in which sustained high performance is possible.
UP NEXT: Postprandial Gastrointestinal Distress as a High-Correlation Biomarker for Systemic Inflammation and Impaired Executive Cognitive Performance
Chronic lower abdominal pain drives systemic inflammation — elevating CRP and IL-6 — that population-level research consistently links to accelerated biological aging, with unresolved visceral and pelvic pathology estimated to add two to five years to biological age through sustained inflammatory burden alone. WholeLiving's Biological Age Estimation Model incorporates this factor directly — your assessment takes under five minutes.
Ready to understand how these factors are influencing your biological age right now? [Take the Biological Age Assessment →]







